
Allied Health Has a Billable Hours Problem
Allied Health is a service industry. Clinicians are revenue generators.
That statement shouldn't be controversial, but it often lands uncomfortably. The commercial model that underpins an Allied Health provider is the same one that underpins a law firm, an accounting practice or a painting business. Revenue is generated by people doing billable work, measured in time, charged at an hourly rate. Lawyers, accountants, engineers, electricians, physiotherapists. All highly skilled professionals. All operating in businesses where the economics come down to the same question: how many hours of productive, billable work can each person deliver in a day?
Every other service industry has a mature, open conversation about this. Allied Health, largely, does not. And that reluctance is creating real problems for financial sustainability and for the sector's ability to advocate for better pricing.
The stigma around KPIs and billable hours in Allied Health is unproductive and doesn't serve us well. The word "KPI" alone triggers defensive reactions. Clinicians are rarely educated on why utilisation matters, and business owners are often reluctant to have direct conversations about it for fear of being seen as exploitative. Part of why I write content like this is to use numbers and experience to chip away at that stigma. The more openly we discuss the commercial realities of Allied Health, the better equipped clinicians and leaders will be to build sustainable careers and sustainable businesses.
Where the sector sits
I recently ran a LinkedIn poll asking what a sustainable daily billable hours target should be for a community NDIS Allied Health clinician.
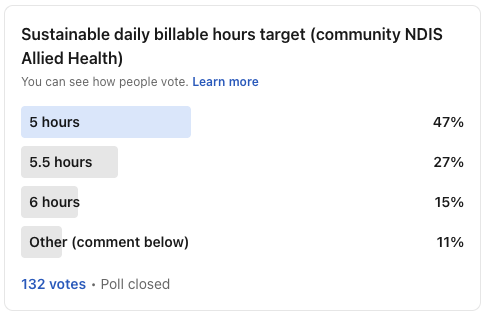
Nearly half the sector believes 5 hours per day is the right target. Only 15% selected 6 hours.
The conversation in the comments was thoughtful and nuanced. Context matters. A new graduate on a complex, geographically spread caseload with no admin support is in a different position to an experienced clinician with a niche focus and a dedicated support team. Setting, experience, caseload complexity, admin infrastructure and funding scheme all influence what's achievable on any given day.
But context can also become a shield. "It depends" is a fair answer to almost any question if you let it be. The uncomfortable reality is that at current charge rates, 5 billable hours per day is becoming very difficult to sustain as a business model. If we can't talk about that openly, the financial pressure will keep compounding.
The maths
Take a community NDIS Allied Health clinician billing at $193.99 per hour across 44 billable weeks per year (the realistic planning assumption once you account for leave, public holidays, sick days and seasonal dips) and a 5-day week.
At 5 hours/day: ~$213,400 per clinician per year
At 5.5 hours/day: ~$234,800
At 6 hours/day: ~$256,100
The difference between 5 and 6 hours per day is roughly $42,700 per clinician per year. Even half an hour extra per day adds approximately $21,300.
For a provider with 10 clinicians, that extra half hour represents over $213,000 in annual revenue. That's more than enough to fund two full-time admin support roles, which would likely free up even more clinical capacity.
Now layer on the NDIS travel pricing changes. Travel is now capped at 50% of the hourly rate. For a mobile clinician billing 4 hours of clinical time plus 1 hour of travel per day, that single change reduces annual revenue by over $20,000 compared to previous pricing. A 5-hour billable day was already tight. Under the new travel arrangements, the margin pressure is significantly worse.
Why margin matters
Before going further, it's worth addressing something directly. When we talk about increasing billable hours or improving margins, the conversation can quickly slide into "providers just want to make more money."
That framing misses what margin actually does in a service business.
Margin is what allows a provider to invest in professional development and clinical supervision for their team. It funds admin support so clinicians can focus on clinical work. It covers the cost of onboarding new staff properly rather than throwing them into a full caseload in week one. It builds the cash reserves to ride out predictable revenue dips during school holidays, public holidays and end-of-year slowdowns.
And right now, margin is what stands between a provider and an increasingly hostile operating environment. I wrote in March about the existential threats facing Allied Health providers in 2026.
Since then, the pressure has only intensified. The NDIS is now central to the federal government's budget savings strategy. The government is moving to weed out unregistered providers. The AFR is running hit pieces on provider invoicing practices, fraud risk in NDIS spending and how scheme funds are being used that signal clearly where political and media scrutiny is heading. Add rising fuel costs and broader economic uncertainty, and the operating environment for Allied Health providers is as difficult as it has been in my career.
A business running at breakeven or thin margins has no buffer to absorb any of this. No capacity to invest in compliance readiness, adapt service models or weather a bad quarter. Margin is not profit extraction. It is the oxygen that keeps a service business running, its team supported and its future viable.
How other service industries compare
Every time-based service industry deals with the same tension: billable hours have to cover the cost of the non-billable hours. What differs is how openly each industry talks about it and what utilisation rate they consider acceptable.
A good mate of mine is a lawyer at a large firm. I've talked with him a lot about Allied Health billable hours over the years. When I explained to him that 5 hours per day was the accepted benchmark, he genuinely could not believe it. In his world, 6 to 8 billable hours is the expectation, tracked in 6-minute increments.
We got away with it because $193.99 was an incredibly high hourly rate, particularly when you consider the volume of NF2F time, travel and kilometres that could be billed on top. The commercial model worked at lower utilisation because the rate was generous enough to absorb it. Times are changing, and rates are, in my opinion, more likely to decrease rather than increase.
Across service industries, international benchmarks sit well above where Allied Health currently operates. The SPI Research Professional Services Maturity Benchmark, which tracks over 400 firms globally across consulting, IT, accounting, engineering and marketing, identifies 75% as the optimal utilisation threshold and a 70-80% range as the sustainable target. In law, the Association of Legal Administrators benchmarks effective firms at 70%+. Note: I couldn't find Australia specific equivalent benchmarks.
Allied Health, at a 5-hour target on a 7.6-hour day, sits at roughly 66%. That's below the floor of what most service industries consider viable.
And the comparison is more generous to Allied Health than it first appears. In NDIS, clinicians can bill for travel time and non-face-to-face (NF2F) work like report writing, session prep and phone calls. I've written before about how much can technically be billed from a single 45-minute face-to-face session. Most other service industries cannot bill separately for equivalent activities. Those costs are absorbed into the hourly rate or written off.
The advocacy problem
The Allied Health sector is actively advocating for higher charge rates through the NDIA's Annual Pricing Review process. That advocacy is important and in many cases well-founded.
But it is significantly weakened when the sector cannot point to a consistent utilisation baseline.
Some providers bill 4.5 hours per day. Others manage 6. Some bill heavily for NF2F. Others charge almost none. There is no widely referenced Australian benchmark for Allied Health utilisation that the sector can collectively point to and say: this is what responsible, well-managed service delivery looks like, and the economics still don't work.
Without that, the pricing conversation becomes very difficult to prosecute. If some providers are demonstrably under-utilising available capacity, the funder's response is predictable: show us you're maximising what you already have before asking for more.
The counter-argument is that documentation burden and NDIS compliance are what cap utilisation. That's a legitimate point. But if the sector wants that argument to carry weight in a pricing review, it needs consistent data rather than anecdotal frustration. Assertion is not evidence, and right now the sector is largely asserting.
The path to credible advocacy runs through credible measurement.
Low utilisation is a leadership problem
If your clinicians aren't hitting billable targets, the first question should be about the conditions you've created for them.
I've written previously about leadership being the difference in Allied Health. The same principle applies here. Your team's output is a reflection of your operational design, your systems and your leadership. Their failures are your failures.
The most common structural reasons clinicians under-bill are all within a provider leader's control.
Clinicians doing admin. Every hour a clinician spends scheduling, chasing service agreements or invoicing is $193.99 in forgone revenue. Compare that to the cost of a dedicated admin person. The opportunity cost is enormous, and this applies to sole traders too. If you're spending two hours a day on admin, you're not saving money. You're losing it.
Poor geographic scheduling. Clinicians driving across a city between appointments because referrals aren't allocated by area. This is an operational design failure.
No commercial onboarding. New graduates are not taught to think about billable hours at university. If you expect them to intuitively understand utilisation, you're setting them up to fail. I've written previously about the financial reality of hiring new graduates: most are running at a loss in Year 1, even in a perfect scenario. Businesses can offer high salary, low billables or phenomenal support. Pick two. That trade-off needs to be understood and planned for, not discovered in the P&L at the end of the year.
Scaling without adjusting structure. A provider with a few billing staff and no dedicated admin can often manage on lower targets. Past a certain point, the overhead structure needs to change. Many providers feel the pinch at exactly this point because they've grown headcount without growing operational maturity.
Inconsistent expectations. A team without a clear target, a way to measure it, a reason it matters and support to get there is a team set up to fail.
This is about designing the business so that clinical time is protected, supported and valued. Not about pushing clinicians more. Work smarter, not harder.
What to measure, and how
My preference for most providers is a flat daily billable hours target, averaged over a fortnight or a month. Everyone knows the number. It's intuitive. And it accommodates the reality that not every day looks the same. A clinician can have a packed Tuesday with back-to-back sessions, then use Friday as a lighter WFH day for telehealth, admin and team meetings. That's fine, as long as the average holds.
I'll be honest: I didn't realise how many providers were tracking billable hours on a daily basis until I started talking about KPIs publicly on LinkedIn. I'd assumed everyone was averaging at least weekly. Daily tracking creates noise, anxiety and pointless conversations about individual off-days. It makes far more sense to tie your utilisation tracking to your invoicing or payroll cycle. If you pay fortnightly, measure fortnightly. It gives a cleaner picture and a natural review rhythm.
The next level beyond retrospective tracking is forward utilisation projections based on what's already booked in clinician calendars. Low utilisation next week is fixable. Low utilisation last week is money you can't get back. If your practice management system gives you visibility on upcoming bookings, use it proactively.
For providers working across multiple funding schemes at different rates, revenue targets give a truer picture of contribution. They're harder to implement and can feel confronting for clinicians, but for providers with the right culture, — they're powerful.
Percentage utilisation is useful for back-end analysis but harder to operationalise as a daily target. 70% of a 7.6-hour day is 5 hours and 19.2 minutes. That’s not a number anyone can work with intuitively. Keep the frontline metric simple.
Billable hours are one metric, not the only one
If billable hours are the only KPI in your business, you're measuring activity rather than performance. Utilisation tells you how much time is being billed. It tells you nothing about whether the work is good or clients are satisfied. Some metrics worth considering alongside billable hours:
Report turnaround times. How long between assessment and report delivery? Delays affect client experience, plan utilisation and referrer confidence.
Progress note completion. Are notes done within your policy timeframe? Late documentation is a compliance risk and often a sign of deeper capacity issues.
Client response times. How quickly does your team respond to enquiries, referrals and communications? This directly influences your referral pipeline.
Net Promoter Score or structured client feedback. Almost no Allied Health provider does this well, and it would be transformative. Billable hours tell you what already happened. Client satisfaction tells you what's about to happen to your referral pipeline, your retention and your reputation.
Outcome measures. Are interventions producing measurable results? This will matter increasingly as the NDIS moves toward outcomes-focused models.
When clinicians feel assessed holistically rather than reduced to a single number, accountability improves and the conversation about targets becomes far less adversarial.
Where to from here
The Allied Health sector needs to get more comfortable with the commercial reality of service delivery. Sustainable clinical care requires sustainable businesses.
That starts with consistent measurement. Know your numbers. Track utilisation properly and be able to articulate where your clinicians' time goes and why. Talk to your peers, talk to advisors, talk to anyone who can give you an honest read on whether your operational model stacks up.
And if billable hours are low, look at the system before looking at the staff. Invest in admin support. Design schedules that protect clinical time. Onboard staff into commercial reality. Set clear, fair targets and give people the conditions to meet them.
The sector's ability to advocate for fair pricing depends on its willingness to demonstrate that it's managing the pricing it already has. That's not a comfortable truth, but it's the foundation that credible advocacy is built on.