
The Existential Threats Facing Allied Health Providers in 2026
Three risks are converging. Most providers aren't modelling any of them. Almost none are modelling what happens when they overlap.

The market is already under pressure
Next time you see a post on LinkedIn or Facebook looking for a clinician in a metro area, watch the comments. Dozens of providers responding within hours, all competing for the same referral. That's the market right now, before any of the changes I'm about to describe have landed.
Metro areas are saturated with Allied Health providers. More are entering the sector every year. Early career clinicians starting businesses. New grads going out on their own as sole traders. Provider numbers keep climbing. At the same time, funding is tightening, participant numbers for key cohorts are being actively reduced and the policy signals are pointing toward fewer dollars flowing through the NDIS for Allied Health. More providers chasing a shrinking pool of work.
That's the baseline. Now add three structural risks landing in the same 12-month window.
If you're the director of an Allied Health business with employees, a commercial lease and fixed overheads — this is the article worth reading slowly.
The sector has its head in the sand
My LinkedIn feed at the start of this year was full of happy new grad posts and "starting a new position" updates. I love the enthusiasm, and maybe I’m cynical (or maybe I’m a realist), but all I could think about was how many of them would last the year out, considering what’s to come.
I'm shocked at the volume of recruiting that is still happening. Chris Antartis (Rebel Recruitment) and I discussed this on our first episode of Allied Health: Live & Unscripted. Chris mentioned that 80% of his clients are still recruiting, hard. In the context of everything I'm about to lay out in this article, that made the hairs stand up on the back of my neck.
When the NDIA cut travel and therapy rates last July, the sector treated it like the sky was falling. Petitions. Open letters. Outrage. That was a drop in the ocean compared to what's on the horizon. Allied Health is a reactive sector. We wait for changes to land, then scramble. The changes coming in 2026-27 are too big for that approach.
People are talking about these risks individually. What I'm not seeing is anyone seriously modelling what happens if the worst case plays out across all three in the same window. That's the gap this article is trying to fill. The providers engaging with this content are a tiny fraction of the sector. The rest have either moved on, burned out from last July's changes, or simply aren't paying attention.
Here's what concerns me most. If things do go wrong, and there are credible reasons to think they will — it's last in first out. The new grads posting excitedly about their first roles are the ones most exposed to redundancy if businesses start downsizing. The enthusiasm is real. So is the exposure. Both things can be true at the same time.
The sector doesn't need more optimism right now. It needs more directors modelling their downside and fewer people pretending the market is stable.
I wrote about these shifts for DSC late last year. That article covered what changed. This one is about what's coming next, and why the compound effect is what people should actually be worried about.
Read: The Future of Allied Health with I-CAN and New Framework Plans
Three risks, one window
Three independent forces are bearing down on Allied Health providers in a compressed timeframe. Each one on its own is manageable for a well-run business. The compound effect is what turns a difficult year into an existential one, particularly for providers that are unregistered, paediatric-heavy or reliant on FCA revenue.
The organisations most exposed are the ones carrying fixed costs they can't unwind quickly. Employees on contracts. Commercial leases with years left to run. Overhead structures built for a revenue base that may not exist next year.
Variable revenue against fixed costs is where businesses fail. I'll cover what to do about it at the end of this article. But first, you need to understand what's coming.
Risk 1: NDIS Pricing — APR & PAPL (July 2026)
Differentiated pricing has been signalled clearly and repeatedly.
The Independent Pricing Committee recommended moving away from one-size-fits-all price limits toward a model that accounts for qualifications, service settings and regulatory obligations. The NDIA committed to a dedicated therapy pricing review to inform that shift. The 2025-26 APR consultation closed in February and the NDIA has committed to releasing recommendations earlier this year.
The question is timing and mechanism. The NDIA has a track record of signalling reform and then delaying delivery. But the IPC report, the dedicated therapy review and the commitment to an earlier APR release this year make the signals more concrete than usual. The possible outcomes range from a standard indexation increase through to differentiated rates based on registration status.
If differentiated pricing arrives, unregistered providers could face cuts while registered providers hold steady or receive an increase. For registered providers, it could be the first time the compliance burden is actually reflected in what they're allowed to charge.
For context, most Allied Health therapy rates haven't seen an increase since 2019. They were frozen for six years, then some were actively cut last July. Everyone saw their travel cut. Providers have been absorbing rising wages, insurance, rent and operational costs against a static or shrinking price cap for the better part of a decade. Any further reduction lands on a cost base that's already under strain.
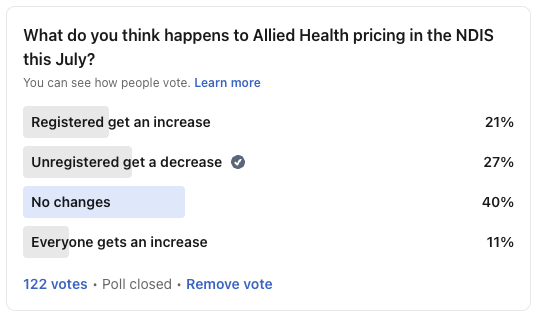
I ran a poll recently asking what people think happens to Allied Health pricing this July. 40% said no changes. 27% said unregistered providers get a decrease. 21% said registered providers get an increase. 11% said everyone gets an increase.
For what it's worth, I think unregistered providers will see a decrease to their NDIS rates this July. The signals from the IPC, the dedicated therapy pricing review and the broader direction of reform all point in that direction. I hope I'm wrong. But I'd rather plan for it and be pleasantly surprised than ignore it and scramble.
Risk 2: FCAs, I-CAN & New Framework Plans (July 2026 onward)
I've written about this at length separately. If you haven't read it yet, I'd strongly recommend it before continuing:
Read: The NDIS FCA Problem Nobody Wants to Talk About
The short version: Functional Capacity Assessments are a significant and reliable revenue line for many Allied Health providers, particularly OT-heavy organisations. They're high margin, demand is built into the planning cycle, and until now there's been no quality threshold that might interrupt the revenue.
I-CAN and the new Support Needs Assessments change that. As standardised assessment tools replace FCAs as the primary planning input under new framework plans, the need for funded, provider-written reports diminishes. Regardless of whether I-CAN is a better or worse approach, the commercial reality is straightforward: a revenue line that many organisations have structured their workforce around is being replaced.
The question is pace. I-CAN won't replace FCAs overnight. But the trajectory is clear, and providers that have built operating models around FCA volume need to be modelling what their business looks like without it.
There's also a broader question the sector isn't asking loudly enough: how will budgets be calculated under new framework plans? We don't have a clear answer yet. But based on the direction of reform, we are more likely to see plans get smaller under new framework plans than bigger. If the assessment tool changes and the budgets shrink, providers lose revenue from both ends.
Risk 3: Thriving Kids (October 2026, full rollout January 2028)
I've covered this extensively in an earlier article that breaks down the Advisory Group report and what it means for Allied Health:
Read: Thriving Kids in 2026: What the Advisory Group Report Means for Allied Health
The core issue: children with developmental delay and autism with low to moderate support needs are transitioning out of the NDIS into a commissioned model. Rollout commences 1 October 2026, with full implementation by 1 January 2028.
If your caseload has a significant paediatric NDIS component, you need to know what percentage of your caseload falls into the Thriving Kids cohort. That's the number at risk.
The replacement pathway, a mix of commissioned services and Medicare, will likely pay less and operate differently. Providers won't be managing individual plan budgets. They'll be working within commissioned structures, potentially at lower rates, with different reporting and accountability requirements. In all likelihood, small Allied Health providers and sole traders won't receive commissioned funding directly. The contracts will go to larger organisations, and smaller providers will either subcontract or miss out entirely.
Additionally, I am hearing from providers that paediatric participants are already getting their plans reduced ahead of the formal Thriving Kids rollout. This is often how NDIS reform works in reality. The policy says October 2026. The operational shift starts well before that, in plan reviews and reassessments, behind the scenes. If you work in early childhood and you've noticed tightening in recent months, you're not imagining it.
The compound scenario
Each of these risks in isolation is manageable. A rate adjustment, a shift in service mix, a gradual transition of a cohort. Providers adapt. That's normal.
The danger is all three landing in the same window.
Take an Allied Health business that is unregistered, does a meaningful volume of FCAs and has a heavy paediatric NDIS caseload. In the space of 12 months, that provider could face:
Rate compression on their therapy services from differentiated pricing or new price controls
Loss of a high-margin service line as I-CAN and new framework plans replace FCAs as the primary planning input
A significant reduction in their largest referral cohort as Thriving Kids transitions low-to-moderate paediatric participants out of the NDIS
Now add fixed costs.
Clinicians on employment contracts. A lease with three years remaining. Admin staff. Insurance. CPD budgets. Software subscriptions. Professional indemnity. None of those costs flex downward when revenue drops. They stay exactly where they are while the top line shrinks.
If that sounds like your organisation, sit with it for a moment. Because that is how businesses go under. Revenue falls gradually, then suddenly, against a cost base that was built for a different market.
You don't need to know the exact numbers to model this. Ranges are more useful. What does your business look like if therapy rates drop 10%? What if FCA revenue halves? What if 30% of your paediatric caseload transitions out? What if it's 50%? Now stack two of those scenarios. Now stack all three.
If you haven't run those numbers, you don't actually know whether your business survives this.
And these three aren't the only pressures
The three NDIS risks above are the structural ones. They change where revenue comes from and how much of it there is. But they land on top of broader cost pressures that are squeezing margins from the other direction.
Payday super takes effect from 1 July 2026. Superannuation will need to be paid at the same time as wages rather than quarterly. For providers with multiple employees, that's a cash flow hit. It doesn't change the total annual cost, but it changes when you pay it. Cash flow timing is what kills small businesses.
Support at Home price caps will affect providers with aged care revenue. We don't yet know where the final price caps will land, but if you've seen how the direct and indirect pricing structure has played out so far, you'll know it's been a debacle. And if you're operating as an associated provider or subcontractor, you're only ever going to see a percentage of the cap anyway. I daresay the caps won’t be as high as we are hoping.
None of these are necessarily existential on their own. But they compound. Every additional cost pressure reduces the buffer you have to absorb the bigger structural shifts.
Cutting headcount isn't the safety net you think it is
If your risk management plan is "I'll make redundancies" or "they're still in probation so it's fine," you need to think more carefully.
First, redundancies cost money. You need cash to make redundancies. Notice periods, accrued leave, potential redundancy pay. Most Allied Health service businesses are extremely cash poor. If revenue is already falling by the time you decide to act, you may not have the cash to execute the very plan you're relying on.
Second, even employees in probation are protected under general protections provisions in the Fair Work Act. The qualifying period for unfair dismissal doesn't apply to general protections claims. If a terminated employee can frame their dismissal as being connected to a workplace right, a complaint or a protected attribute, you have a claim to respond to regardless of how long they've been employed. Norelle Pratt's recent post breaks this down for clinic owners.
The risk here has increased materially. Fair Work Commission lodgements have grown over 70% in three years driven in large part by employees using AI tools to draft and file claims. The FWC President has publicly acknowledged that AI is enabling people to file claims who wouldn't have previously had the knowledge or resources to do so.
This matters for directors because the cost of responding to a claim, even one that ultimately fails, is real. Legal fees. Management time. Disruption. And under the Fair Work Act, costs orders against unsuccessful applicants are rare. You wear the cost of defending the claim regardless of the outcome.
If your response to revenue pressure is "I'll cut headcount quickly," make sure you understand the legal exposure that comes with it. Get proper advice before you act, not after.
And if you're thinking a contractor-heavy model protects you, think again. If those contractors are really employees in substance, which is common in Allied Health, you're exposed to sham contracting claims, back-payment of entitlements and penalties. If they're genuinely independent, they have no obligation to stay. When the market tightens, they can walk to another provider tomorrow with no notice and no handover. Either way, a contractor-heavy workforce isn't a risk shield. It's a different set of risks.
Which providers are most exposed?
The three risks don't hit everyone equally. The organisations most vulnerable are the ones that are generic, undifferentiated and competing on availability alone.
Be honest with yourself for a moment. What is your brand? What makes you different from the practice down the road?
Most Allied Health providers are unremarkable. Generic marketing with stock photos. Same vague promises about holistic, client-centred care. In a growing market, that was fine. There was enough work to go around. In a shrinking market, where metro providers are fighting over a reducing pool of referrals, being forgettable is a liability.
When Thriving Kids lands, the strategic choice for paediatric-heavy providers is clear: diversify or double down. Both are legitimate.
I covered this in detail here: Thriving Kids in 2026: What the Advisory Group Report Means for Allied Health
But if you're going to double down on paediatrics, you need to own it. Be the provider that schools call first. Be the name GPs remember. Be memorable enough that when commissioning arrives, you're already the obvious choice.
I shared a video last week about Glue Store closing after 27 years despite $100m in revenue, whereas Culture Kings sold for $600m. The difference was identity, not scale. A specialist paediatric provider with deep school relationships and a reputation for outcomes has options when the market shifts. A generic business that happens to see a lot of kids does not.
That principle extends across all three risks. A registered provider with strong governance and clear positioning is set up for differentiated pricing. An unregistered, undifferentiated organisation is exposed on every front. A few years ago, having capacity and “no waitlist” was enough to differentiate you. The market is now so saturated with unremarkable providers that availability alone means nothing. Why would a referrer, a school or a family choose you?
The compound risk hits hardest where there's nothing holding the business together except volume.
What to do about it
If you're a director, this is on you. Running a business is managing risk. If you have employees and a commercial lease, the risk sits with you personally. Your name is on the lease. Your assets are on the line. Nobody else is going to model this for you (Well, I can 😉)
Start now. Not after the APR lands. Not after I-CAN rolls out. Now.
Do a proper risk analysis. If you have a governance framework, you should have a risk register. If you have a risk register, these three items should already be on it. If you don't have either, that tells you something about how prepared your business is for what's coming.
I've written about why governance matters here: What Is Governance and Why Should Allied Health Providers Care?
Map your revenue exposure. Break your revenue down by service type (eg. FCA vs therapy vs other) and cohort (eg. paediatric vs adult vs aged care vs private). You need to see where your concentration risk sits before you can manage it.
Model the downside. This is the part most people avoid because it's confronting. Do it anyway. Run 10%, 20% and 30% reduction scenarios for each of the three risks. What does your business look like if therapy rates drop 10%? What if FCA revenue halves? What if 30% of your paediatric caseload transitions out? Now stack two. Now stack all three. Identify which combination creates a viability problem. Be honest about the numbers.
Stress-test your fixed cost base. At what revenue level does your business stop being viable? How far can the top line drop before you can't cover your lease, your payroll and your overheads? That number is your floor. If you don't know it, you're not managing risk. You're just hoping.
Decide deliberately. Diversify, specialise or restructure. All three are valid responses. What isn't valid is doing nothing and hoping the market stays the same. The market has told you, in published government documents, that it's changing. The question is whether you adapt on your terms or on someone else's.
The bottom line
The Allied Health market is already competitive. It's about to get significantly more so, with fewer funded participants, tighter pricing and more providers competing for what's left.
The providers who come through 2026-27 will be the ones who looked at the downside scenario, ran the numbers and made decisions while they still had choices. The ones who didn't will be the ones explaining to their accountant how it happened so quickly.
If you can't answer the questions in this article about your own business, you're already behind.
Need help modelling your exposure?
If you want to stress-test your business against these scenarios, I work with Allied Health directors to:
Map revenue concentration and identify where risk sits
Model downside scenarios across pricing, FCAs and cohort transition
Build or update risk registers as part of a broader governance framework
Develop practical, staged responses before reform lands
Book a 20-min strategy call here: conwaygroup.com.au/appointments