
Thriving Kids in 2026: what the Advisory Group report means for Allied Health, and practical ways to respond
Commissioning, education integration and where value is shifting

Pressure on the NDIS, particularly in early childhood, has been building for some time. What has been less clear is what comes next.
The Thriving Kids Advisory Group Final Report, released alongside Mark Butler’s 3rd February 2026 press conference, provides the clearest view so far of how Thriving Kids is intended to operate. Together, the report and the Minister’s remarks move the policy from broad intent to a nationally agreed model, with shared design principles, confirmed funding and an implementation timeframe.
Thriving Kids was first announced publicly in August 2025, with an initial rollout date of 1 July 2026. The latest announcements confirm that timeline has shifted. The model has been agreed in principle by National Cabinet, backed by $4 billion in funding, with rollout commencing on 1 October 2026 and full implementation by 1 January 2028, as outlined in the Minister’s media release.
While significant operational detail is still to come, the overall direction is now much clearer. The conversation has moved from whether Thriving Kids will happen to how it will be implemented and how Allied Health services, such as occupational therapy, speech pathology and physiotherapy, will fit within the emerging system.
Much of the report will feel familiar. In many respects, it formalises patterns that have already been playing out:
sustained pressure on the NDIS, particularly in early childhood
persistent workforce constraints
growing discomfort with travel-heavy 1:1 therapy models
increasing frustration from schools and early childhood education and care services about how supports are delivered
This article is not about reacting with alarm or rushing to overhaul your business. It is about understanding the intent of the reform and thinking calmly and practically about what it is likely to mean for Allied Health providers over the next few years.
What problem Thriving Kids is trying to solve
At its core, Thriving Kids responds to how early childhood support has evolved in practice, rather than how it was originally designed.
Over time, the NDIS has become the default access point for children with developmental delay and autism, including many with low to moderate support needs. For families, this has often felt like the only realistic way to access timely and affordable support. For providers, it has meant the NDIS absorbing a cohort it was not designed to serve at scale.
Government commentary consistently points to the way current settings have shaped service delivery. Diagnosis has increasingly functioned as a gateway to funded support and therapy has often defaulted to direct intervention with the child — rather than broader support for families, educators and everyday environments.
These patterns are best understood as the result of system incentives rather than individual clinical decisions. Over time, however, they have contributed to structural pressures that are now difficult to ignore.
In practice, this has included:
inconsistent access and long waitlists
significant geographic variation in service availability
workforce strain driven by travel-heavy, low-leverage delivery models
families coordinating multiple unconnected providers
growing disruption reported by schools and ECEC services
From a government perspective, the system has also become harder to oversee. While individual children may benefit, there is limited visibility of whether current settings are improving outcomes at a population level, reducing future support needs or delivering value for public investment.
This is the gap Thriving Kids is designed to address.
The reform aims to create a clearer pathway for children with low to moderate support needs outside the NDIS, while preserving the NDIS for children with permanent and significant disability. The intent is not to reduce support, but to organise it in ways that are easier to access, coordinate, evaluate and scale.
Seen this way, Thriving Kids is less about withdrawing services and more about reshaping how early childhood support is structured and delivered.
What the Thriving Kids model proposes
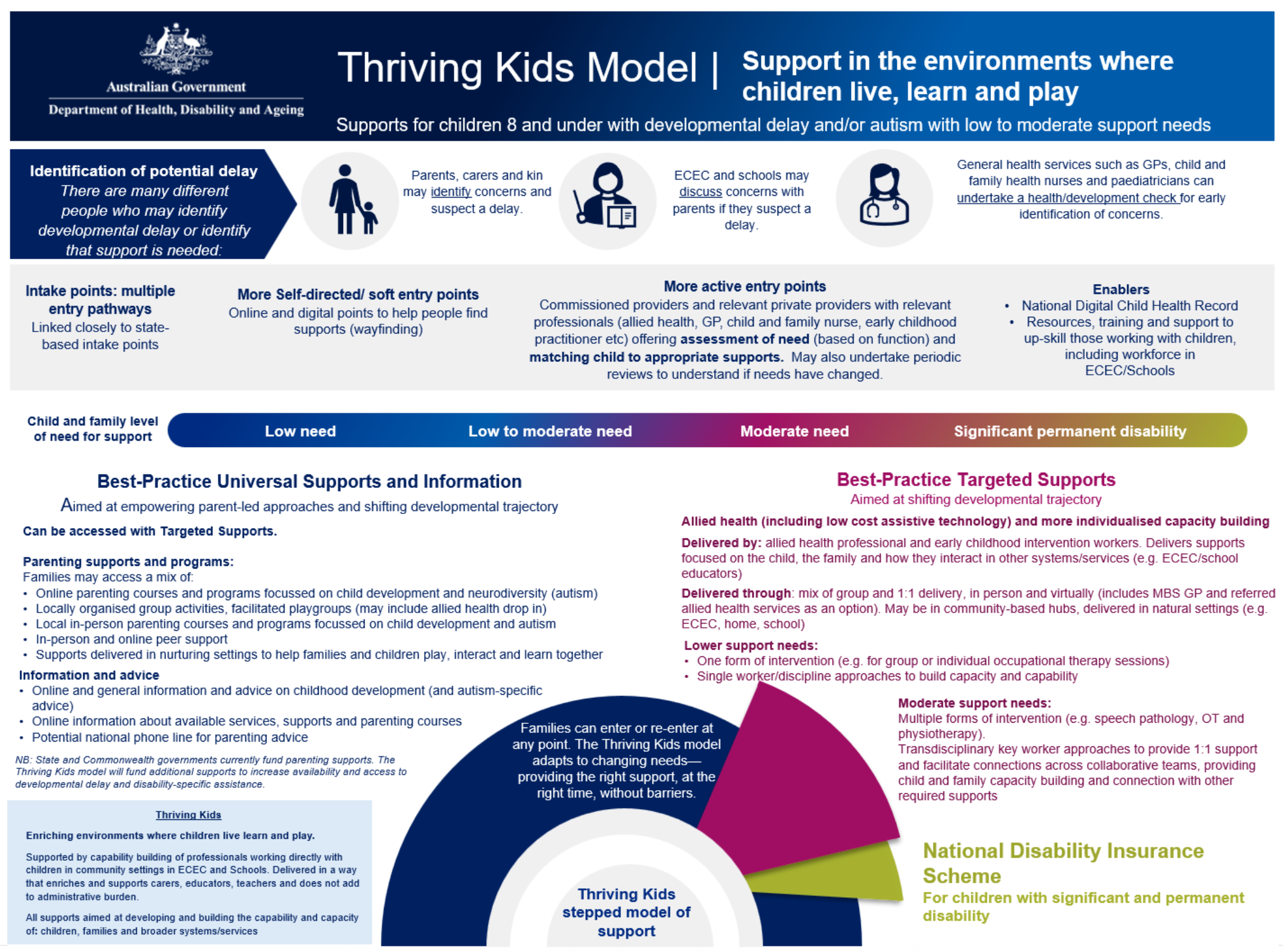
Source: Page 9 of the Thriving Kids Advisory Group Final Report
Thriving Kids shifts the centre of gravity away from therapist-led intervention toward parents, educators and everyday settings, with Allied Health playing a supporting and enabling role rather than being the sole delivery mechanism.
The model introduces a nationally consistent approach built around commissioned services. Children and families are connected to supports that match their level of need and are delivered by providers funded to operate locally. At a system level, this represents a shift from an open, plan-driven market toward a more structured model that prioritises access, coordination and integration.
Commissioning as the primary mechanism
Under Thriving Kids, support for children with low to moderate developmental needs is no longer primarily organised around individual funding packages. Instead, services are commissioned to deliver defined supports within local communities, with families connected to those services rather than managing funding themselves.
This has several implications:
providers are funded to serve a population, not just individual clients
access is less dependent on a family’s ability to navigate funding systems
coordination and consistency become explicit design goals
Medicare as a complementary pathway
Medicare sits alongside this model, rather than replacing it.
GP referrals may connect families either to commissioned Thriving Kids providers or to a capped number of Medicare-funded allied health services. This creates a hybrid pathway that supports access without reverting to a fully individualised, fee-for-service model as the default for early childhood developmental support.
The Key Worker model
Where children are supported by multiple providers, the model recommends a Key Worker approach.
In practice, this means one clinician may act as the main point of contact for the family and help coordinate supports across providers and settings. This is not intended for every child and does not require a separate, dedicated role. It is a coordination function that can sit within an existing clinical role where appropriate.
The intent is to reduce fragmentation, not add another layer of complexity.
A shift in where and how support is delivered
A defining feature of Thriving Kids is its emphasis on everyday settings, particularly early childhood education and care services and schools.
Rather than relying primarily on children being withdrawn from class for individual therapy, the model places greater emphasis on:
clinicians working alongside educators
coaching and supporting staff
building capability within existing environments
This reflects increasing concern from education settings about disruption to learning, administrative burden and the volume of external providers entering schools under current arrangements. It also signals a preference for models that integrate support into existing systems rather than operating alongside them.
Outcomes designed in from the start
Outcomes and evaluation are embedded into the model from the outset.
Thriving Kids is explicitly designed to generate better visibility of what is working at a system level, not just for individual children. Funding, service design and delivery models are expected to evolve over time based on evidence about impact and effectiveness.
Taken together, the Thriving Kids model points toward a system that is:
more structured
more locally organised
more integrated with education
less reliant on individual funding packages as the default
What this means for Allied Health providers
Demand is shifting, not disappearing
For Allied Health providers, Thriving Kids does not signal the end of demand. It does signal a shift in where value sits and how services are expected to be delivered.
The most significant change is that early childhood Allied Health, including services such as occupational therapy, speech pathology and physiotherapy, is becoming more clearly segmented.
Children with permanent and significant disability will continue to sit within the NDIS. Children with developmental needs that are lower to moderate, changing or time-limited are increasingly being directed toward alternative pathways. Over time, this reduces the NDIS’s role as the default growth engine for early childhood Allied Health, particularly at the lower end of the support continuum.
Delivery models and workforce use are under pressure
Alongside this segmentation, policy settings are placing greater pressure on delivery models that are expensive to run or difficult to coordinate. From a commissioning and education system perspective, highly mobile, travel-heavy 1:1 therapy models create friction. They are harder to scale, harder to integrate with schools and ECEC services and harder to justify at a population level.
Many of these models emerged to solve real access problems, particularly in areas with limited local services. The shift underway is not a judgement on clinical quality. It reflects a change in how governments and education systems are seeking to organise support at scale.
Workforce impact is also being treated as a deliberate design consideration rather than an unintended consequence. Governments have been explicit that Thriving Kids will change where and how Allied Health capacity is used, with states taking a greater role in coordinating delivery rather than relying on an open market of individual providers entering schools and centres independently.
This aligns with what many schools and early learning services have been signalling for some time:
fewer providers involved with each child
better coordination across supports
less disruption to classrooms and routines
What providers may notice before formal rollout
While Thriving Kids is not scheduled to commence until October 2026, with full implementation from January 2028, large system reforms rarely arrive without some movement ahead of formal start dates.
In practice, providers may notice changes in how early childhood supports are interpreted or applied in the lead-up to implementation. Anecdotally, this can include greater scrutiny of ongoing supports for children with lower to moderate needs, increased variability in plan decisions or a more cautious approach to renewals.
These patterns do not constitute formal implementation of Thriving Kids, and they are not consistent or universal. However, they reflect the way systems often begin to shift behaviourally before structural change is complete. This is one reason why waiting for perfect certainty can leave providers reacting late rather than adapting gradually.
Where value is increasingly sitting
As a result, local presence is becoming more valuable than geographic reach. Providers who are embedded in communities, have established relationships with schools, ECEC services and GPs, and can work across settings without excessive travel are better aligned with the direction of reform.
Over time, this is also likely to sharpen the distinction between cohorts:
children with higher needs who require intensive, individualised intervention
children with low to moderate needs who benefit more from coaching, coordination and capability building
Allied health expertise remains central in both cases. What is changing is how that expertise is applied. Increasingly, value is created not only through direct therapy hours, but through how clinicians support families, educators and environments to respond effectively to children’s needs.
Practical steps providers can take now
Thriving Kids will not be fully implemented for some time. However, waiting for final guidelines before thinking strategically increases risk.
There are a number of steps providers can make now that align with the direction of reform, regardless of final commissioning detail.
1. Reduce concentration risk
Providers with a heavy reliance on NDIS-funded early childhood work are more exposed to reform risk.
This does not require abandoning paediatrics or losing a specialist identity. It requires being intentional about where risk sits, rather than inheriting it by default.
In practice, this may include:
diversifying revenue beyond NDIS early childhood
strengthening private or clinic-based services for families who can afford them
developing clearer, program-based offerings rather than open-ended therapy
expanding into adjacent cohorts or funding streams where appropriate, such as older children, adolescents, adults, aged care, or private, insurance and employer-funded work
Diversification creates optionality. Optionality matters in reform periods.
At the same time, specialisation remains a valid strategy. Some providers will choose to double down on paediatrics and focus on being exceptional within a clearly defined niche. A strong reputation with families, schools and future commissioners can be a defensible position.
The distinction is not diversification versus specialisation. It is intentionality. Understanding the risks you are carrying and choosing them deliberately matters more than the specific path taken.
2. Develop lighter-touch, scalable models
Thriving Kids favours models that support more children without defaulting to long-term, high-frequency 1:1 therapy for low to moderate needs.
Providers should be testing and refining approaches such as:
parent education and coaching models
short programs and groups
hybrid or digital supports where appropriate
These models tend to be easier to commission, easier to evaluate and easier to integrate with education settings.
3. Re-think how you work with schools and ECEC
One of the clearest signals in the report is concern from schools and ECEC services about the volume and disruption associated with external providers.
Providers who want to remain welcome in education settings should be strengthening models that focus on:
coaching and training educators
supporting classrooms rather than withdrawing children
establishing communities of practice with schools or early learning services
This represents a shift from delivering therapy in schools toward supporting schools to meet children’s needs within everyday environments.
4. Reduce reliance on travel-heavy delivery
Highly mobile 1:1 models are resource-intensive and increasingly misaligned with commissioning and education preferences.
Practical steps may include:
consolidating service locations
shifting more delivery into clinics or local hubs
reducing reliance on models where travel time is absorbed by clinicians, subsidised through therapy margins, or inconsistently funded
This is about reducing travel as a structural cost rather than asking clinicians or families to absorb it. It also reflects family and system preferences for services that are predictable, coordinated and easier to sustain over time.
5. Strengthen local relationships and partnerships
Thriving Kids is designed to operate through communities rather than individual transactions.
Providers should be investing in relationships with:
local schools and ECEC services
GPs and child health services
community organisations and councils
not-for-profits likely to be commissioned
For some providers, future opportunity may sit in partnerships, consortium arrangements or subcontracting rather than holding contracts directly.
6. Build coordination and capability-building skills
The model places greater emphasis on coordination, coaching and system-level impact.
Providers should be building capability in:
key worker or coordination functions
working across disciplines and settings
coaching families and educators
supporting environments, not just individuals
These skills are likely to become increasingly valuable as commissioning expands.
7. Clarify your value proposition
Providers should be able to answer, in plain language:
Why would a school, a family or a commissioner choose you?
If the answer relies primarily on availability or willingness to travel, it is becoming less durable. Clarity around outcomes, approach, expertise and fit matters more as competition and commissioning increase.
8. Start measuring what matters
Even basic outcome tracking creates an advantage.
This does not require complex systems. It does require being able to articulate:
what changes as a result of your involvement
how families, educators or environments are better supported
why your approach creates value
9. Prepare administratively, without over-investing
Some light preparation makes sense:
ensure Medicare provider numbers are in place
understand likely referral and commissioning pathways
capture outcomes in ways that can be communicated clearly
This is about readiness, not racing ahead of policy detail.
A final perspective
Thriving Kids does not sit in isolation. It aligns with broader reform across I-CAN, New Framework Plans and the increasing emphasis on outcomes, evidence and public value in funded systems.
The Advisory Group report and accompanying Ministerial commentary reduce uncertainty about direction, even while implementation detail continues to evolve. While delivery will vary by state, the core model has been endorsed and is intended to proceed.
The message for providers is not that Allied Health is less important. It is that the way support is organised, funded and delivered is changing.
Commissioning, stronger integration with education, reduced reliance on individual funding packages and greater emphasis on coordination and capability building will shape where demand flows and which models are favoured over time.
The most useful question is not whether Thriving Kids is good or bad policy. It is:
How exposed is my current model to the direction of reform, and where do I want to be positioned over the next few years?
There is time. Implementation is staged and detail will continue to evolve. Providers who adapt gradually, test new models, strengthen local relationships and clarify their value proposition will have more options as Thriving Kids moves from design into delivery.
Allied health remains essential. The systems around it are evolving. Providers who recognise that early will be better placed to continue doing meaningful, sustainable work with children and families.
Thinking through what this means for your organisation?
If you are considering what Thriving Kids could mean for your organisation, service mix or risk exposure, I work with Allied Health providers to:
test current service and workforce models against reform direction
identify concentration, sustainability and transition risks
clarifying strategic options around diversification or specialisation
translating reform intent into practical, staged next steps rather than reactive change
Book a strategy call here: https://www.conwaygroup.com.au/appointments