
The NDIS Bill has landed. Here's what's actually in it for Allied Health providers.

The Securing the NDIS for Future Generations Bill was introduced to Parliament yesterday. After months of signalling and the 2026-27 Budget on Tuesday night, the legislation is on the table.
For Allied Health providers, the immediate question is what changes and when. The longer question is what the government has actually written down about Allied Health in the supporting documents.
I covered the build-up in Butler's NDIS warning shot, laid out the structural pressures in the existential threats facing Allied Health providers in 2026, and posted the headline read on the budget itself on Wednesday morning. Today is the practical version. What's in the Bill, what it means, what to do.
What's in the Bill
The Bill is split into five schedules covering access and planning, fraud and integrity, governance and pricing, new framework planning rollout and transitional provisions.
For Allied Health, the changes that matter most sit in Schedule 1 (access criteria, budget resets, the new evidence test, the tighter impairment link, unscheduled reassessment limits) and Schedule 3 (Minister-set pricing, differentiated pricing for unregistered providers, automated decision-making).
These changes phase across multiple dates between 7 days after Royal Assent and 1 January 2028 (see timeline below).
The Bill text and Explanatory Memorandum are on the Parliament of Australia website. The Department's About the changes page is the plain English version.
The Impact Analysis appended to the Explanatory Memorandum is also worth reading. It contains the actual numbers and the government's policy case for each change.
What the Impact Analysis says about Allied Health
The most consequential material for Allied Health sits in the Impact Analysis. This document forms the second half of the Explanatory Memorandum and is where the government has documented its case for each measure.
On capacity building daily activity [CBDA] budgets, the Impact Analysis is very direct. From page 204:
Four claims are doing the work in that passage.
First, NDIS therapy funding sits well outside the norm for comparable Commonwealth programs.
Second, CBDA budgets are growing too fast.
Third, capacity building isn't reducing need over time the way it was supposed to.
Fourth, the published research evidence for high volumes of long-term therapy is thin.
Whatever you think of those claims, this is the argument now sitting in a Cabinet-approved policy document. For Allied Health to push back effectively, the sector needs to disprove these claims with data and evidence. The sector's current advocacy posture is largely qualitative. The government's case is quantitative. Until those two registers meet, the outcomes from each reform round will keep landing the same way.
The big changes for Allied Health providers
The Department published its reform timeline alongside the Budget. It is the clearest single view of when each change starts.
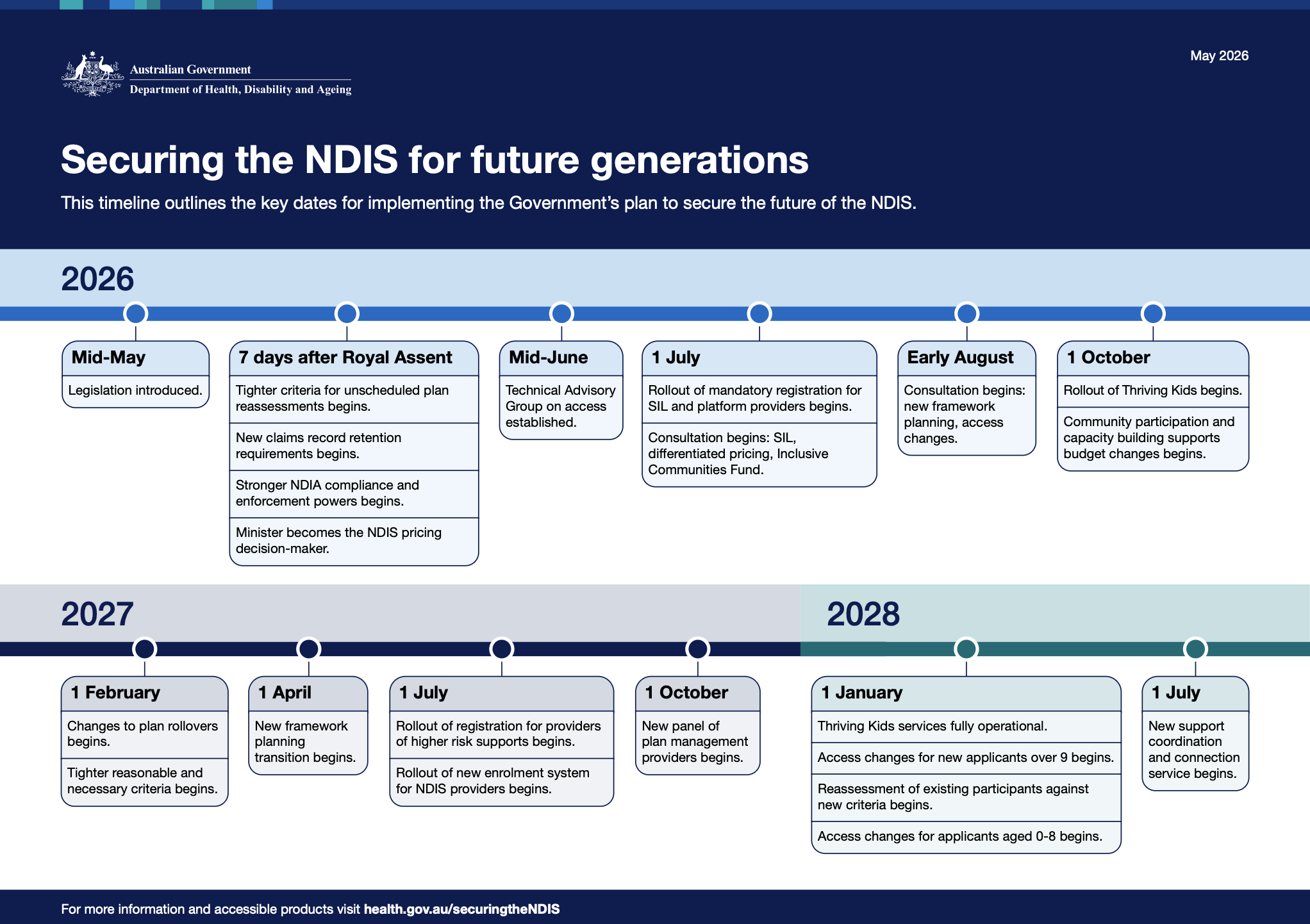
What follows is the practical detail behind those dates.
CBDA budgets are being cut by 10 per cent (from 1 October 2026)
Capacity Building Daily Activies [CBDA] is the line item that funds therapy supports for the vast majority of NDIS participants. Budgets are being cut by 10 per cent. The cut phases over twelve months from 1 October 2026 as plans are reassessed or renewed.
99 per cent of NDIS participants have CBDA funding (p. 204). For children aged 0 to 8, every participant has CBDA and it makes up around 69 per cent of their total plan (p. 233). The 9 to 14 cohort also has 100 per cent CBDA coverage at 42 per cent of plan. Paediatric-heavy providers across the 0 to 14 age range are the most exposed.
The Impact Analysis is also explicit about expected market impact: "The impact on the allied health or therapy provider market is not expected to create significant employment or provider viability shocks, especially given there is latent unmet demand across the care and support economy" (p. 238). The government's view is that displaced therapy workers can move into Aged Care Support at Home, veterans' care and Medicare. That substitution assumption deserves scrutiny.
The actual percentage will be set by the Minister after the Bill passes, which means the figure can be adjusted later in either direction.
Thriving Kids changes paediatric Allied Health (from 1 October 2026)
Running alongside the CBDA reduction, the government is rolling out Thriving Kids. From 1 October 2026, the program begins providing supports for children aged 8 and under with developmental delay and low to moderate autism support needs outside the NDIS.
From 1 January 2028, NDIS access arrangements for this cohort change. New applicants aged 0 to 8 with developmental delay or autism and low to moderate support needs will be directed to Thriving Kids rather than the NDIS. Children with permanent and significant disability, and children aged 0 to 8 with developmental delay or autism and high support needs, will continue to be eligible under usual NDIS arrangements.
The Department's stated position is that existing 0 to 8 participants in this cohort will continue to be reassessed under the eligibility criteria in place before 1 January 2028. The detail will sit in transitional rules.
Thriving Kids is the largest single eligibility lever in the government's stated target of reducing scheme participation from around 760,000 to 600,000 by the end of the decade, a 160,000 reduction.
This is the most significant structural change for paediatric Allied Health providers in years. I analysed the policy design earlier in the year when the Advisory Group report landed, and the most recent state development is NSW choosing not-for-profits to deliver the program, a decision that has not landed well with private practices.
Combined with the CBDA reduction landing on the same cohort, paediatric-focused providers need to think hard about caseload mix and the next two years of revenue.
Foundational supports beyond Thriving Kids
Thriving Kids is the first tranche of Foundational Supports. Per Minister Butler's 3 February 2026 press conference, the overall commitment by governments to Foundational Supports back in 2023 was $10 billion.
$4 billion of that is now committed to Thriving Kids over five years, split $2 billion Commonwealth and $2 billion states and territories. $1.4 billion of the Commonwealth's $2 billion will be direct funding to states for delivery.
$6 billion remains for further Foundational Supports yet to be designed. The Minister has flagged the next priority cohort as adults with severe and chronic mental illness, an estimated 230,000 people identified by the NDIS Review as having significant unmet need.
The Second Reading speech also flagged a separate $200 million Inclusive Communities Fund to rebuild community organisation capability so participants have non-NDIS options for community participation.
The shape and timing of the further supports will be agreed through the National Agreement on Foundational Supports between the Commonwealth and states and territories. The design decisions over the next 12 to 24 months will determine whether the further tranche lands as an alternative service stream Allied Health can deliver into, or as work routed through channels that exclude private Allied Health providers.
Unscheduled plan reassessments are getting much harder (from seven days after Royal Assent)
Only participants, plan nominees and guardians will be able to request an unscheduled plan reassessment. Providers and support coordinators no longer can. The NDIA also gets longer (up to 90 days) to decide whether to do a reassessment. Reassessments will only be granted where there has been a significant and ongoing change in support needs or circumstances.
The Impact Analysis is direct on the government's reasoning: "There are currently no limits on who may request a plan reassessment which has resulted in providers making these requests, despite the potential actual or perceived conflict of interest, or where there is no evidence of a change in circumstances" (p. 201). Around 25 per cent of plan change cases were initiated by support coordinators (p. 201). Average plan inflation from unscheduled reassessments ran at 21 per cent in 2025 (p. 200), with the Minister citing an average plan increase of 20 per cent per reassessment in the Second Reading speech.
This is a fair criticism of how parts of the sector have been operating. A common pattern has been functional capacity assessments and reassessment reports written by Allied Health providers that recommend more therapy hours from the same provider. That workflow is contracting hard. Providers and support coordinators can no longer initiate requests, and the criteria for granting a reassessment are tighter. The Impact Analysis estimates monthly unscheduled reassessments will fall from around 12,000 to between 5,000 and 6,000 (p. 240). Reports will still be needed when participants themselves request a reassessment, but the volume of provider-led report writing, and the revenue attached to it, will drop substantially. I've written about the dynamics of this market in the NDIS FCA problem nobody wants to talk about.
Reasonable and necessary is being tightened from multiple angles (from 1 February 2027)
The Bill rewrites the reasonable and necessary test in several material ways at once.
The new evidence hierarchy is the most discussed change. The NDIA must consider, in order: published, peer-reviewed and generalisable research; evidence of the support's effectiveness given the participant's circumstances; evidence of how the participant has responded in previous plans; and other matters the agency considers appropriate.
The provision that does the real work lets the agency refuse funding where there is limited or no published research backing the support, even where the clinician's case for that individual participant is strong. Reports built primarily on clinical observation will face a structural problem, as will any therapy modality with limited published evidence at the population level.
Three other changes tighten the test alongside the evidence hierarchy. The CEO must consider whether comparable supports are available at a lower cost. The CEO must be satisfied the support is not more appropriately provided by another scheme or government service system, meaning therapy that could be delivered through Medicare, Aged Care Support at Home or state health systems is more exposed. Scheme sustainability is now a principle the CEO must have regard to.
This applies whether the report supports an access request, an unscheduled reassessment or a routine plan renewal.
The Minister can set caps on therapy hours (from 1 February 2027)
Therapy hours currently sit in individual plans, based on what the planner agrees is reasonable and necessary, informed by clinician reports. The Bill adds a new override. The Minister can make a rule setting caps on funding, hours or worker-to-participant ratios for any support or group of supports, applying to participants generally or to a defined group of participants.
In practice the lever shifts from plan-by-plan decisions to caps that apply across whole groups. The Minister could cap therapy for a specific discipline at 20 hours per year for all participants under 8, for example, regardless of what individual clinician reports recommend. The Explanatory Memorandum example (p. 51) has a planner determining 30 hours per discipline is reasonable and necessary for a participant, with a group cap then limiting the plan to 25 hours. The cap applies even where it does not meet the actual cost of supports.
Cap levels will be set in further rules made after the Bill passes.
The new rule about supports "directly arising" from impairment (from seven days after Royal Assent)
Supports must directly arise from the participant's eligible impairment. This sounds technical and the practical effect is narrower funding for therapy programs that address downstream effects of an impairment rather than the impairment itself.
For example, a participant accepted into the NDIS for one impairment who also has secondary issues may find it harder to fund therapy that addresses the secondary issues unless they can be tied directly to the eligible impairment.
Differentiated pricing is coming, and it has many levers
The Bill enables differentiated pricing across a much broader set of dimensions than just registration. The Minister can set different prices based on whether a provider is registered, the qualifications or experience of the practitioner, the region where supports are delivered, the intensity of the support, whether delivery is in-person or via telehealth, the time of day or day of the week and whether services are individual or group. That is a wide range of levers.
The Impact Analysis notes there are around 82,000 CBDA providers in the market and only about 9,000 are registered (p. 238). The registered versus unregistered split is the most operationally significant axis for Allied Health, and the breadth of the power means margin pressure could come from multiple directions over time.
Most therapy providers will face a registration decision in the next 12 to 24 months.
Plan management and support coordination are being commissioned
The Bill sets up a panel arrangement for plan management. The government will commission a panel through competitive procurement, with deeds intended to be in place by 1 October 2027. The Bill also enables a ban on plan managers providing any other NDIS supports.
Support coordination is being commissioned through a separate model, with the government directly commissioning providers to deliver a new support coordination and connection service from 1 July 2028.
Support coordination is the bigger structural change for Allied Health. A large share of therapy referrals currently runs through support coordinators. When the function is directly commissioned, independent support coordinators who have built warm referral networks with Allied Health providers will be replaced by commissioned providers operating to procurement-defined standards. Providers relying heavily on support coordinator referrals should audit and reduce that dependency now.
The APR hasn't landed yet (and the process will change moving forwards)
Separate to the Bill, the NDIA's 2026-27 Annual Pricing Review is due in the coming weeks. The APR is what sets actual hourly rates for the new financial year. Therapy rates have been frozen since 2019.
Whether the APR moves therapy rates this year will materially affect provider margins. The Bill moves formal pricing decision-making to the Minister once Schedule 3 commences seven days after Royal Assent, so the 2026-27 APR is likely the last one finalised under existing Agency-led arrangements. From 2027-28 onwards the Minister will make the pricing determination based on Agency advice.
The permanence test is being tightened (from 1 January 2028)
An impairment will not be considered permanent unless three things hold: the person has undertaken all appropriate treatment, no other treatment is likely to materially improve or alleviate the impact, and the impairment is likely to persist for the person's lifetime regardless of treatment.
Appropriate treatment is defined as treatment that is evidence based, regularly undertaken in Australia and can reliably be expected to improve, reverse or alleviate the impact. A person's personal and environmental circumstances, including financial and geographical access to treatment, are not relevant. The Soo example in the Explanatory Memorandum (p. 64) makes this concrete. A five-year-old with bilateral moderate hearing loss on a waiting list to see an ENT specialist is found ineligible because she has not yet had evidence-based interventions like grommets. Wait times in her regional area are not a consideration.
For paediatric providers, this layers on top of Thriving Kids. Even where a child is not diverted to Thriving Kids on the developmental delay or autism test, the permanence test may still rule out NDIS access.
Eligibility will now consider access to other service systems (from 1 January 2028)
The Bill adds a new access requirement. A person must have at least one impairment that is not an "excluded impairment." Excluded impairments are those caused by a motor vehicle accident or work-related injury that may be addressed by workers' compensation or motor vehicle accident compensation schemes. Where all impairments fall in this category, the person will not meet NDIS access.
The Minister can also prescribe additional service systems and impairments as alternative supports through NDIS rules that require agreement of all states and territories. The Explanatory Memorandum flags aged care and some chronic health conditions as examples. If aged care is later declared an alternative support, the NDIS to Aged Care Support at Home boundary tightens further.
What to do next
Model what your NDIS revenue looks like under a 10 per cent CBDA reduction. Crude but effective as a starting point. The 10 per cent applies to participants who remain on the scheme. Paediatric providers have compounded exposure since the Thriving Kids transition will sharply reduce new entry to the scheme from 1 January 2028.
Audit and reduce reliance on support coordinator referrals. The commissioning of support coordination from 2028 will reshape the referral channel structurally. Providers with diversified referral sources (direct, GP, NDIA partners, self-referral) will be much better positioned.
Make the registration decision deliberately. Differentiated pricing for unregistered providers is coming. Decide whether your business will register or accept differential pricing, and start the work now if registration is the path.
Update the evidence base for your reports ahead of 1 February 2027. The new evidence hierarchy elevates published research and absence of published research alone can be grounds to refuse funding. Reports built primarily on clinical observation will need to integrate published evidence to hold up.
Track what gets announced after the Bill passes, along with the APR. The Bill is the framework, and the actual percentages, prices and intensity rules will be set later.
What comes next
The compound effect is what matters most. CBDA cuts, the evidence test, the alternative supports test and the support coordination commissioning combine into a different operating environment for Allied Health. Providers who plan against the whole picture will get to better decisions faster than those working through each change in isolation.
The changes phase over roughly 30 months, from seven days after Royal Assent through to 1 January 2028. Providers who start positioning now have time to shape their response. Those who wait for the Rules and pricing determinations to land will be making decisions under pressure.
Parliamentary debate continues from here, with submissions from the disability community and peak bodies likely to shape the final form. Rules, pricing decisions and support determinations will be developed over the second half of 2026 and into 2027.
I'll be writing more in the coming weeks. Several threads in the Impact Analysis are worth pulling on their own, including the compound risk picture for paediatric Allied Health, the registration strategy decision and what the new evidence test means in practice.
If you want to talk about what this means for your business, I'm happy to have a conversation.