
NDIS billing for Allied Health in 2026-27: rules, grey areas and risk
What the new line items change, where the rules already answer the question and where genuine grey areas remain.

The era where you could bill the NDIS more or less how you liked is ending, and increased scrutiny is coming.
This is my interpretation, built on consulting to more than 100 providers, previously running a national Allied Health business that supported 10,000+ participants across 10 disciplines, and countless hours watching how the sector talks to itself online. Much of what this article contains is contested. I have had most of these debates already and I am happy to have them again. I am not here to tell you what to do. Do whatever you want. The aim of this piece is that, for whatever you decide to do, you are making a more educated and informed decision.
I covered the 2026-27 price moves and the six new line items in my breakdown of the Annual Pricing Review, so I will not repeat the mechanics. This is about the decisions that sit on top of them, and what happens if you get them wrong.
Why I am writing this
In the current NDIS environment, the pressure is real and none of it is the provider's fault. Budgets are shrinking, therapy prices are frozen or cut and the cost of running a business keeps climbing. When margin gets squeezed the rational instinct is to recover it somewhere, and the nearest lever is the participant. Push the travel charge up. Add a block of non-face-to-face (NF2F) time to each session.
We have watched this play out once already. After the NDIA halved the hourly rate for provider travel last July, NF2F claiming rose. The Agency surveyed how providers structure their sessions, named session structure a policy issue in the Annual Pricing Review (p.94) and from 1 July split NF2F into its own line item. The lever providers reached for is now the thing under the microscope.
It comes down to risk
For most of the Scheme's life the NDIA has been close to blind on how money is spent. At the National Press Club in April, Minister Butler put a number on it. The Agency cannot see the evidence behind around 90% of claims, which is why every provider is being moved onto a digital payments system, and it expects 90% of payments to flow through registered providers under expanded mandatory registration. I covered what the speech means for Allied Health in my article here.
The new line items are another mechanism for the Agency closes that visibility gap. Once travel, telehealth, report writing and NF2F each sit on their own line, it can read how much of each is claimed, by whom and in what proportion. The data it has lacked for a decade starts arriving in July.
That is what changes the calculation. For years providers could bill more or less how they liked, with little visibility and little consequence. Every claiming and pricing decision now carries a risk, and the risk is rising. Some of what follows is settled by the rules and some sits in genuine grey, though a lot of what gets defended online as grey is not actually grey. The documents already answer it. Whatever you decide, decide it knowing the risk you are carrying.
Also, the "dodgy, greedy NDIS provider" narrative applies to Allied Health too, whether we choose to accept it or not. Delivering a clinical service does not exempt us from the rules that apply to every other provider when delivering a public, taxpayer funded service.
Find the margin inside your own business first
The honest starting point is your own operating model. Utilisation across the sector is too low and too much time is lost to non-billable work. I have written separately on the billable hours problem and on what a layer of middle management costs. Plenty of providers cannot get clinicians to five billable hours a day, then look to participants to recover the shortfall. This is simple: margin comes from increasing revenue or cutting expenses, and you should work both. Look first at the revenue you can lift inside your own business, like getting your team to bill more of their available hours, before you charge participants more.
Billing for what you actually do
This is where the new line items put claiming under the most scrutiny, and where the rules are clearer than the online debate suggests.
NDIA requested reports
What counts as an NDIA requested report causes a lot of confusion, so it is worth going to the source. The term is not new. It has sat in the Pricing Arrangements (PAPL) for years, and the definition turns on the purpose and content of the report rather than on who asked for it. A report counts as NDIA requested if it is required at the start of a plan to set goals, at review to measure outcomes against those goals or to make recommendations about ongoing needs. Functional Capacity Assessments, Assistive Technology assessments, home modification reports and progress reports will often meet that definition.
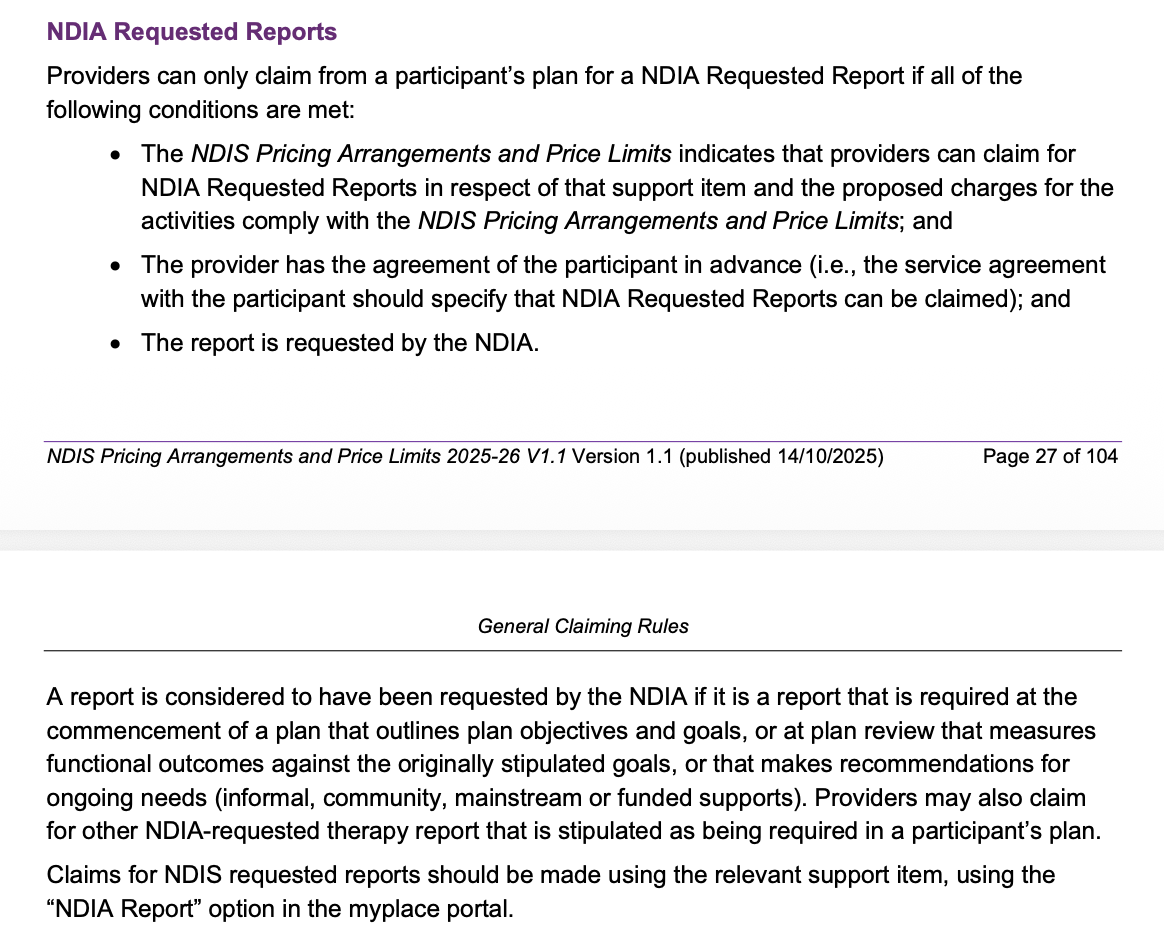
PAPL 2025-26, p.27-28
What is new for 2026-27 is that report writing sits on its own line, separate from direct service and general NF2F. This is where correct billing starts to matter beyond the single claim. Bill report writing and NF2F accurately and the data shows how much skilled indirect work therapy involves. Bury report writing inside a generic NF2F block and the data understates it, which weakens the evidence base for every future pricing decision about it. Billing the right line is an act of advocacy for Allied Health as much as an act of compliance.
NF2F time
Let me be precise about the concern, because this is where I’ve copped the most heat recently!
NF2F time has real value. A great deal of skilled Allied Health work happens around the participant rather than directly with them. Interpreting assessment data, designing a program, writing to a school or a co-worker, genuine case work on a complex participant. That work is essential and it takes what it takes. Report writing and complex indirect work tied to a participant's goals are legitimate and should be charged.
The concern is narrow and specific. It is the routine flat block, a set amount of NF2F bolted onto every session and billed whether or not that time was spent on that participant.
The strongest defence of the flat block runs something like this. Billing each transaction is an administrative burden, clinicians will not record it well and the management overhead to police it eats the margin it protects. So providers set an average, and many spend more time than they charge across a caseload, which feels like a fair trade in the participant's favour. I understand the logic and I have sympathy for the operational reality behind it.
It still does not survive the PAPL. The conditions for claiming NF2F are explicit:
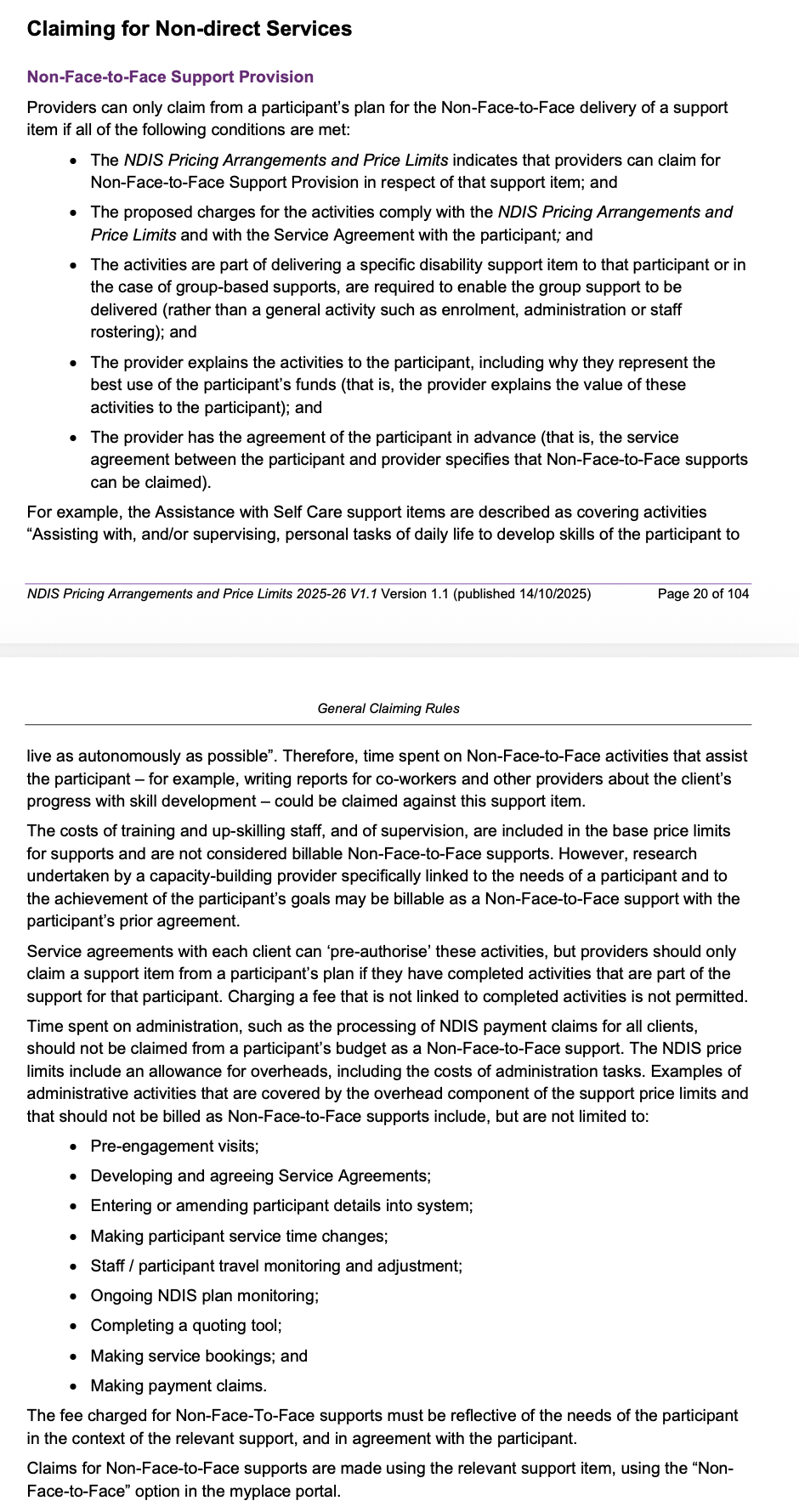
PAPL 2025-26, p.20-21
The activity must be part of delivering a specific support to that participant. The provider must explain why it represents the best use of the participant's funds. The participant must agree in advance. Then come the lines that decide it. The fee "must be reflective of the needs of the participant in the context of the relevant support". Providers should only claim "if they have completed activities that are part of the support for that participant". And in plain terms, "charging a fee that is not linked to completed activities is not permitted". The same section puts supervision, training and routine administration inside the base price overhead, where they are not billable as NF2F at all.
So the plain reading is this. Billing a flat amount of NF2F on every session, where the clinician did not spend that time on activities for that participant, is not compliant with the PAPL. The averaging defence does not rescue it. An average is built across a caseload but the rule applies to the participant. A participant who needed ten minutes this fortnight is billed for thirty, and is subsidising the participant who needed forty-five. They are paying for time not spent on their goals, which is the exact thing those conditions rule out.
The compliant approach is the simple one. Charge for the time you actually spend on that participant's NF2F work. A complex participant might take forty-five minutes of preparation one week and fifteen the next. A stable participant might take ten minutes a fortnight. Bill that, and make sure you have evidence (a progress/case note).
Why I think NF2F is the next price target
This is an informed prediction and I could be wrong. Look at how the NDIA justified the travel cut last year. It gave two reasons. Travel claims could exceed the value of the support to the participant, which is a value argument. And travel time need not carry the on-costs built into direct care, which is a cost argument. Apply either to routine NF2F and the direction is not hard to read. The three-year pricing workplan names differentiated pricing and billing integrity as focus areas for the 2026-27 Therapy Pricing Review, and the new line items are how the evidence gets gathered. A lower price for NF2F and telehealth than for face-to-face is a potential next step. Budgets sit under the same pressure as prices, and with session structure already named a policy issue in the APR, the cost and value of each separate therapy line item will keep being reviewed.
If your financial model assumes routine NF2F holds at this rate and volume, treat that as a risk to plan around.
What you can ask a participant to pay
The second category is about what you ask a participant to pay beyond the plan.
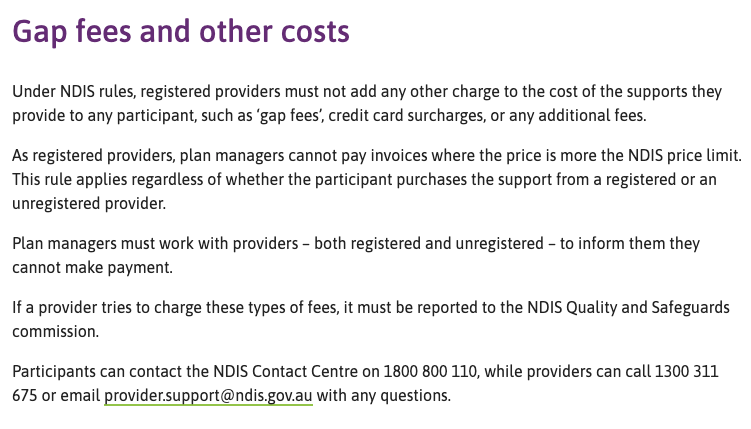
Gap fees
Gap fees are the most contested and grey area in NDIS billing right now, and the recent price cuts have made them more tempting. For example, the Other Professionals rate dropped from $193.99 to $156.16, the gap between a provider's private rate and the NDIS rate widened, and more providers started weighing whether to charge the difference.
If you are a registered provider you cannot charge above the price limits, full stop, including for self-managed participants.
So the gap-fee question really only arises for unregistered providers, and there it turns on how the participant's plan is managed. A self-managed participant has no price cap, so a rate you both agree to is between you and them.
The contested case sits in between, an unregistered provider and a plan-managed participant.There the practice is specific. You bill the plan manager the NDIS rate, which is all it will ever pay, then invoice the participant separately for the gap. The plan manager only sees the capped amount, so the debate is about that second invoice.
The NDIS guidance is where the grey comes from. It says registered providers must not add gap fees, and that plan managers cannot pay above the price limit whether the provider is registered or not. It does not squarely address an unregistered provider privately invoicing a plan-managed participant for the difference, and some providers have been told directly by the NDIS provider support team that it is fine. Even the line saying these fees must be reported can be read as pointing back to registered providers, since that is who the ban names. That is the argument. Providers have been reported and investigated for the practice regardless.
For what it is worth, I wish the NDIA would settle this properly and close the loopholes, because the ambiguity leaves providers guessing and participants exposed. There is a shelf life on it either way. With mandatory registration expanding and the intent for 90% of payments to flow through registered providers, the day registration becomes mandatory for you is the day the question disappears, because a registered provider cannot charge a gap at all.
Then there is the risk, and it goes well beyond an invoice being knocked back. A single complaint can trigger a Code of Conduct investigation, a referral to the Agency's fraud team and a hold on your payments while your billing is reviewed more widely. For a business that runs on Scheme cash flow, that is the real exposure.
People will push back on this, and some will keep charging the gap, because the grey is real and the wording is unclear. Wherever you land, weigh the risk against what the gap actually recovers.
Travel charges
Travel is an example of a genuine grey area, and the confusion starts with the price list itself.
You will see the provider travel non-labour item priced at $1.00. That figure is a notional unit, not a per-kilometre rate or a cap. You claim the dollar value of the cost in units, so a $12.50 toll is claimed as 12.5 units. The item carries no price limit at all, which is why "you cannot exceed the price limit" does not settle this the way people assume. There is no price limit on this item to exceed.
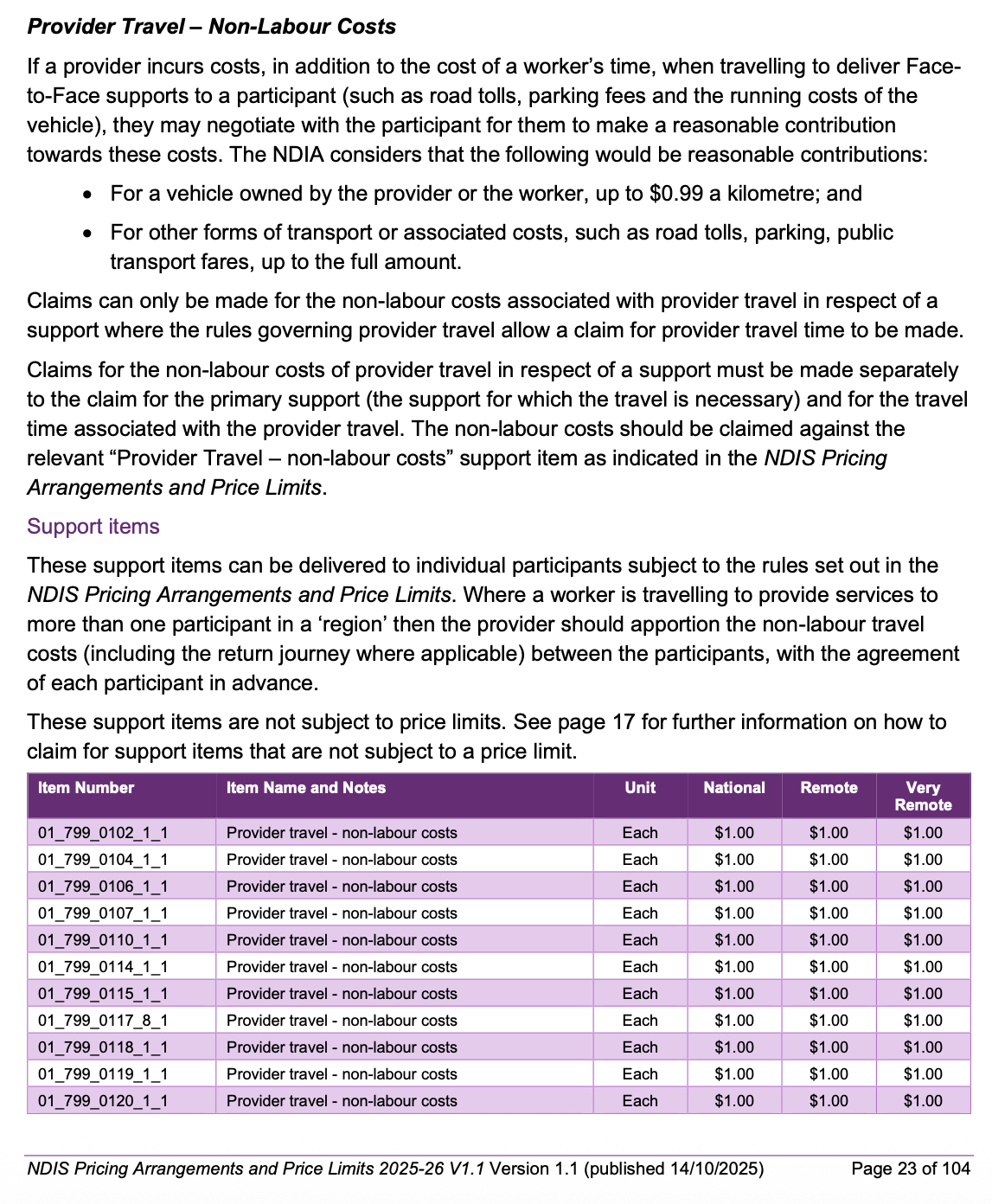
PAPL 2025-26, p.23
What the PAPL sets instead is a reasonableness standard. When a provider incurs vehicle running costs travelling to deliver face-to-face support, they may negotiate a reasonable contribution from the participant, and the NDIA considers a reasonable contribution to be up to $0.99 a kilometre for a standard vehicle. The higher per-kilometre figures you may have seen quoted apply to vehicles modified for accessibility, or to transporting the participant in the community, which is a different support to a clinician driving to a home visit.
So here is the honest position. Technically you can agree almost any contribution, especially with a self-managed participant or through a service agreement, because the item has no hard cap. The $0.99 is what the NDIA considers reasonable for a standard vehicle, so a charge above is contentious with the Agency's own line on fair pricing. Expect scrutiny, and weigh the relationship risk as the market tightens.
Actual cost does not automatically make a charge reasonable. Just because you drive a diesel that costs more to run, there is a fair question about why the participant should carry that. When fuel prices spiked, some providers lifted their rate to $1.30 or $1.50 a kilometre on new service agreements. The instinct is understandable. However, the call is yours, and it is worth weighing what it recovers against what it risks.
The consequences
The Code of Conduct applies to every provider, registered or not. Accepting public money brings you inside it, whatever your registration status. The Commission recently wrote to 270,000 unregistered providers putting them on notice, and it has named strengthened oversight and regulation of unregistered providers and sole traders as a regulatory priority. Its powers reach unregistered providers too, and include banning orders and civil penalties.
The machinery I describe in the gap fees section sits behind every billing decision here. A complaint can trigger an investigation and a hold on your payments while it runs. The scale of future enforcement is a genuine unknown, but the direction of increased scrutiny on NDIS payments is undeniable.
The bottom line
A commercial case sits underneath all of this. Your relationships, your reputation and your referral pathways are worth far more than the margin any of these levers recovers. Lose a participant worth a few thousand dollars a year over a travel or NF2F charge, or damage the relationship with a referrer who sends you several of them, and the maths turns against you fast.
So decide deliberately. Understand whether the rules settle a decision or leave it grey, and know the risk you are carrying either way. In a tightening market, the providers who run efficiently and ethically are the ones who will still be standing.
If you want help working through what this means for your business, book a discovery call.