
What does a Team Leader actually cost your Allied Health business?
And what does a sustainable model look like?

Most Allied Health providers I come across have a similar story. Clinicians want career progression and the business wants to retain them, so leadership roles get created. Then you look up and realise there are more leaders than the team can financially sustain and not enough clinicians for each of them to manage.
I see it constantly: Team Leaders managing a handful of clinicians each, multiple leaders with reduced caseloads across relatively small teams. The support those leaders provide is valuable, but every Team Leader on a reduced caseload represents revenue the rest of the team has to cover. Very few providers have actually done the maths.
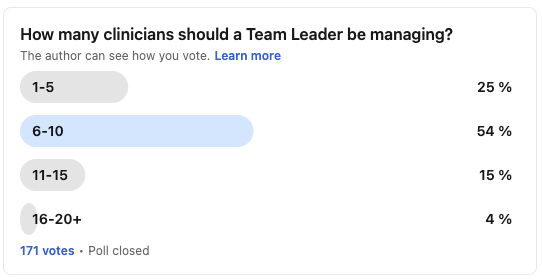
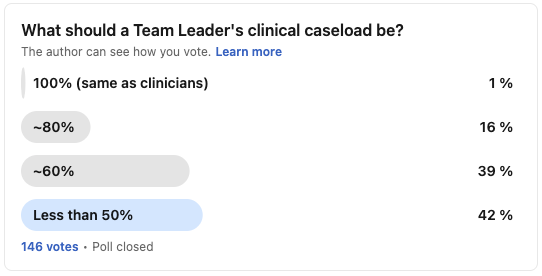
I recently ran two LinkedIn polls on this. The first asked how many clinicians a Team Leader should manage. The second asked what their clinical caseload should be.
The overwhelming theme in the comments was "it depends." I agree. There is genuinely no single right answer here, and the best model for your business will depend on your own circumstances, structure and funding mix.
The intent of this article is to help providers make more educated and informed decisions about their leadership structures. To do that, you need to understand the numbers.
The cost of a reduced caseload
I've written before about why margins matter and how billable hours work in Allied Health, and the same principles apply directly to the Team Leader question.
The numbers below use 5 billable hours per day (25 hours per week) as the baseline, which is where most of the sector currently sits. As I've discussed previously, 5 hours is becoming unsustainable for any provider operating at scale or carrying leadership overheads, but the numbers in this article use it because it reflects the current reality.
Here's what different Team Leader caseloads look like at $193.99 per hour across 44 billable weeks. The red line is the breakeven point: the fully loaded cost of a Team Leader on a $110,000 base salary (roughly $165,000 at a 1.5x multiplier, which covers salary, super, WorkCover, insurances, devices, subscriptions and other unavoidable employment costs). This is what a Team Leader needs to bill just to cover their own employment cost, and anything below that line means their revenue falls short of what it costs to employ them.
Breakeven sits at approximately 19 hours per week, about 77% of a standard clinician target. Every hour per week off the tools costs roughly $8,500 in annual revenue.
Note: This is a gross margin view that covers direct employment cost only. It doesn't include other business expenses like admin support, rent, bookkeeping, CPD allowances, incentive payments, director wages or shared overheads. The real threshold for a Team Leader to be contributing to the business, rather than being subsidised by it, is higher.
To be clear, I'm not suggesting every Team Leader needs to be at or above breakeven. Some roles are worth the investment because of the value they create. The point is that providers should be making that decision deliberately and with the numbers in front of them.
These figures use a $110,000 salary and 5 billable hours per day as an example. To see where your own Team Leaders sit, plug your real salaries and caseloads into the Allied Health Margin Calculator.
Now combine the two poll results. Most respondents said a Team Leader's caseload should be less than 50%, and they should manage 6-10 clinicians. That's a Team Leader costing the business $60,000-$80,000 more than they generate annually while managing a relatively small team. Multiply that across two or three Team Leaders and the rest of the team has to cover $150,000-$250,000 just to sustain the leadership structure.
Operational leadership versus clinical supervision
The Team Leader role typically combines two distinct functions. The first is operational leadership: caseload management, KPIs, performance conversations, burnout and wellbeing, onboarding, work-life balance and day-to-day problem solving. The second is clinical supervision: case reviews, clinical reasoning, competency assessment and professional development.
These require different skill sets and different time commitments. Combining them in a single role is common, but the operational work tends to crowd out the clinical, the Team Leader burns out from constant task-switching, and neither function gets done well.
Clare Batkin from Your OT Tutor recently ran a poll on this.
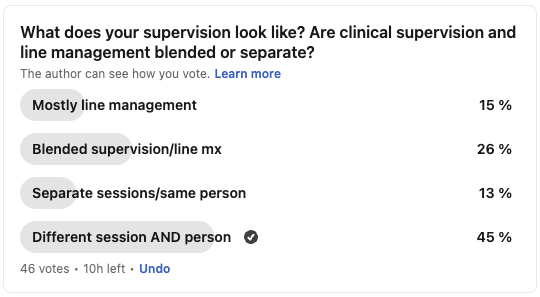
A significant proportion of respondents are still in blended or mostly-line-management setups where clinical supervision gets deprioritised. As Clare noted, better clinical supervision tends to improve the competence and efficiency issues that drive most operational conversations in the first place.
Some larger providers have addressed this by splitting operational and clinical leadership into separate career pathways. If you're too small to split the roles, at minimum separate the sessions even if the same person runs both, and protect the clinical supervision time. Without that clarity, the operational often wins.
The top-heavy trap
A business promotes a clinician to Team Leader because they've been there a few years and want to progress. Then another. Then another. Before long, a team of 20 has four or five people in leadership roles, each on a reduced caseload, each managing a small number of clinicians. The intention behind every one of those decisions was sound, but the cumulative financial impact is often devastating.
Clare also ran a follow-up poll asking whether there are too many Team Leaders in Allied Health or not enough.
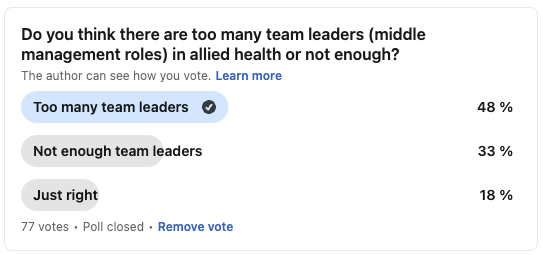
The issue is often less about the number of leaders and more about what they're actually contributing. Clear delegation of responsibility and defined reporting lines for each function make a bigger difference than headcount alone. Bloated middle management kills Allied Health businesses (and any service business for that matter).
In my old business, I ran a 20:1 ratio: one Team Leader managing 20 clinicians on a 60% caseload. I know that is an outlier because we operated at scale, and I built systems from the start with the deliberate goal of keeping the leadership team as small as possible. The Team Leader's role was strictly operational, while clinical supervision sat with a separate layer of senior clinicians who maintained full caseloads.
I'm by no means suggesting 20:1 is the right number for providers. The point is that span of control is a design choice, driven by the systems you have in place, the clarity of the role and what you're actually asking the Team Leader to do. If your Team Leader is the system, if they're the person everyone comes to because there are no documented processes or admin support, then a small span of control might genuinely be the ceiling. That's a systems problem to solve, and leadership is the variable providers control.
Career progression without caseload reduction
One of the biggest drivers of top-heavy structures is the assumption that career progression requires a reduced caseload. Project ownership, mentoring, student supervision, clinical governance contributions and skills-based pay increments can all support progression and retention without reducing billable output. The key is formalising these pathways so clinicians can see a trajectory. If the only visible step up is "Team Leader with fewer billable hours," that's what everyone will aim for.
It's also worth acknowledging that some clinicians are better off working clinically. They got moved into operational leadership because they'd been around for a few years, or because they thought it was the only way to progress. We should be championing and remunerating exceptional clinicians just as much as good operational leaders, and the best Allied Health businesses I come across do both.
The award is changing too
The Fair Work Commission's HPSS Award gender-based undervaluation determination introduces a new classification structure from 1 October 2026, with four further annual increases through to June 2030. The Level 2 classification captures clinicians who provide clinical guidance to less experienced staff or day-to-day supervision to other health professionals, allied health assistants and students. Under Phase 1, Level 2.1 attracts a minimum base salary of ~$96,500 before other entitlements. These descriptors apply well beyond senior staff. Clinicians as early as their second year out of university are commonly providing this type of guidance and supervision, and if they're performing Level 2 work the classification may apply regardless of job title.
This is general commentary only and does not constitute legal or HR advice. If you are unsure how this determination affects your team, get proper employment law advice.
Where to start
Every provider should be able to answer one question about every leader in their business: what is this role costing and what is it delivering in return?
Review your billable targets and utilisation. A 5-hour daily target leaves very little room for leadership overheads, and every fraction of an hour matters these days. If your clinicians' utilisation isn't where it needs to be, the Team Leader cost problem compounds.
Know your ratios. Have a deliberate view on how many clinicians each leader should manage and what caseload they should carry. Make it a conscious decision with the maths behind it.
Separate the functions. Even if the same person does both operational and clinical leadership, separate the sessions and protect the clinical supervision time.
Calculate your breakeven. Every provider should know the caseload at which each Team Leader covers their loaded cost. My margin calculator is a good starting point.
Invest in systems. Strong SOPs, onboarding processes and admin support mean a Team Leader spends less time firefighting and more time on the work that actually makes a difference.
Build multiple career pathways. Create alternatives to caseload reduction and champion great clinicians, not just great managers.
Support your operational leaders. Operational leadership is a skill that doesn't come naturally to most clinicians promoted into these roles. It needs training, support and deliberate development.
If you want to talk through any of this for your business, book a strategy call.
General commentary only. This does not constitute legal, HR or financial advice.